What the HealthTech?! – Giving Control Back to the Practice
This week on What the HealthTech?!, Hayley Levene speaks to the Founder & CEO of iatro, Thomas Porteus. iatro partners with Primary Care organisations to deliver digital health solutions that empower, support, and connect. In this episode, Hayley and Thomas discuss the importance of digital access and communication within the NHS and best practices.
Hi, What The Health Tech listeners. I’m your host this week, Hayley Levine. This is the podcast where we tackle some of the trending topics, ideas, and best practice in health and social care this week. We’re joined by Thomas Porteus, founder of iatro.
Thomas is a passionate advocate for primary care, working with practices to control and manage demand, making sure that all patients can find and access digital services.
Welcome to what the Health Tech, I should tell our listeners me and Thomas go way back, and we used to work at EMIS Health together. So how’s it been since EMIS Health?
It’s been a crazy journey for us. I loved my time at EMS, loved my relationships with practices and lots of good colleagues there, but a brilliant time for me to move on and start iatro and, and solve some of the challenges that, that we’ve been really, really keen to do.
Yeah. You, you look like you’ve been doing really, really well, but obviously a bad time with a COVID. How has that been?
So, I mean, so we, we decided to start the business three months before COVID really hit and primary care has been hit harder than most of the NHS when it comes to Covid.
So, you know, on the face of it, tons of challenges for us engaging with customers, but actually for the products that we’ve been working on it and delivering have been really, useful for COVID.
So while it’s been difficult in places, it’s also been really rewarding to be able to help and make a difference. And some of that’s been COVID specific projects doing appointment booking and some of those, those kinds of projects, but some of it has just been being able to there for practices and saying, look, we know what’s going on and we’ll help you communicate that to your patients and, and, and make sure the message that you want to get out there is really getting out. So, super rewarding for us.
I can imagine. Well, I’m going to talk to you a bit more about the business and, and all the recent awards you’ve been winning as well, which is great. but essentially the main kind of topics I’m going to speak to you about today, the importance of digital access, patient communication, all that quite challenging, actually for practices, and for the health and social care world in general. Talk to me a little about iatro, where did it come from? Where did the idea come from? What do you do to help?
So I think, early on in my career, I was involved in lots of new digital health tools. So, I witnessed the birth of video consultations and econsultations in the UK and saw those early startups on their journey.
And the thing that was, that was always the issue around adoption was it doesn’t matter how much money the NHS spends on it. It doesn’t matter how much practices are told to use something. If patients can’t find and use it without causing a problem for the practice, then it’s not going to get out there. If it doesn’t get out there, it doesn’t get renewed. And if it doesn’t get renewed, that innovation doesn’t bet in.
So there was a really big issue for us around actually most patients can’t find the services that are already being delivered. And that was a massive challenge. We saw that really coming into COVID, you know, news was changing so fast. What service do I use? You know, there’s 15, 16 appointment booking apps, which one can I use? Which one can I use today? Which one can I use today for this appointment? Really, really difficult for practices, for patients.
So, you know, that was where we started Pactice365. We call it our website builder, but that’s really what that’s aboutis helping practices have that level of tool set that any, any business would, because these are challenges that don’t exist for businesses, you know?
Yes, they’re in the business of selling and e-commerce, but the challenges are the same.
And actually as a small business, I know that I can find lots of agencies that are willing to help me with that. I can find lots of free tools. I can find lots of low cost, monthly online applications to help me with that stuff. But that doesn’t exist for practices. So they always get a raw deal.
And then, you know, the small practice team sizes, the management teams, or maybe 6, 5, 6, 7 people max, that knowledge isn’t embedded in there. So how do they manage to do that communication out of band without the help of someone like us to help them do that? So really, really important for us to keep pushing that for them.
Why do you think that, patients have such a problem finding information that they need, how to book an appointment, for example?
So, you know, even in the last three years, the commissioning structure has changed a few times. Practices are completely willing to adopt technology. And I think compared to other sectors within the NHS – you look at the rollout of electronic health records, full stop. Primary care has been a hundred percent digitalised for a long while, and you still got hospitals, you know, with paper on trolley. And digitalization is about putting back codes on paper.
You know, primary care has been really willing to adopt, but because of that and the pace of the change, you know, things change really quick, suppliers are pushing out changes, and that is the practice manager’s job. You know, the MD of the practice to communicate all that to patients across multiple channels. There’s not the time that exists for that.
So we do the work working with other suppliers to package the information about their solutions. So it can go into the websites, it can sign post the patients at the right point for what they want to do in a much cleverer a way. And that’s you know for us, it’s about giving control back to the practice. It’s not about those telling them what they need. It’s about us listening and making sure that comes across.
So one of the big things we do around that is letting them schedule content. And that can be things like, well, I’ve got Sunday afternoon. Now I’m going to put on the bank holiday messages on for the rest of the year, but that’s also taking content on and off each day.
So actually I might be signposting to extended access outside of, you know, outside out of hours and making sure patients can get there.
But the equity of access is really important. So, you know, practices are working in these structures with primary care networks who all have the same services that are being commissioned across that area.
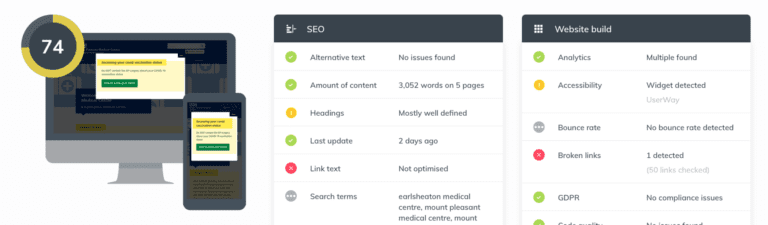
But, you know, we do audits of websites across PCNS sometimes. And we’ll find really big banner on the homepage on one practice and extended access is a sub bullet point bullet point on a contact me page that’s, you know, a bit messy and out of date. And suddenly, even though that, that, that service has been commissioned and that same a digital service has been commissioned. Your access between patients is vastly vastly different just because how well it’s been signposted, you know, and that takes constant constant effort practices.
So I can imagine obviously practices across the whole NHS. They are so busy. They have patients to see they have multiple different priorities. So, so you, when you speak to a practice and say, this is really important, the likelihood is that that will be bottom of the pile and they won’t really, it’s not that you don’t want to understand cause they want to help patients. It’s just that there’s so many other priorities to handle. So how do you deal with those kinds of challenges? So we spend a lot of time reminding practice managers that the one thing that they’re really, really good at is comes, even if they don’t realize it, so we encourage them to think less about the channel, think less about, is it an SMS?
Am I sending a letter and think about the message rather than the format. And at the very least, if it’s on there in text, then that’s great. That’s, that’s, that’s really accessible. It’s great for patients that can get the message for staff. So we encourage them to do more, not less. And that may even be it just doing a little bit.
So you talked about like suppliers and other suppliers and how they handle things. And on your website, you say that the NHS deserves better. Is that what you mean? Or is there something else that you feel?
So fundamentally I think the NHS deserves better, but more than that, I think primary care organisations deserve better.
So, you know, there’s a lot of crossover in those, those kinds of customers where the legacy has been quite disjointed as small organizations who are now kind of rolling up organisations quite often, especially in the primary care market. We’ll start with a nice bit of innovation, roll that out to a nice level of market share within primary care.
And then one of two things happen. They get really big external investment and then really stopped listening to what the customers want and start growing, trying to grow into another market like secondary care, because now they’re on that rat race to get that growth, which doesn’t really give primary care anything it needs.
So you get products that are good enough, but aren’t equivalent to a similar thing under the market.
You know, I spend a lot of time maybe being dismissive of some of the innovation that’s going on in the NHS, because it’s no different than anywhere else. So, econsultations, fantastic. We’ve got really great econsultation product in OneContact, that also does outbound management, but, I spend a lot of time tell people that forms are forms are forms are forms. There is no difference between the way that we’ve technically built that platform for primary care and how you build it for any of the sector.
So these are challenges, inbound, consumer demand. How do you manage inbound consumer demand? This is a story that’s been told in every other vertical it’s happened in banking. It’s happened in travel, you know, it’s happened everywhere else. Companies come into primary care said, well, yes, but it’s a bit special. Well actually, and that, you know, that hurts practices because practices then feel actually, I don’t know how to deal with this. Where as actually, you do know. So, you know, a question we get asked quite a lot when we’re, when we’re talking about one contact and the consulting sessions is like, well, what do I do if someone fills out that isn’t a promotion, well, what do you do if you get a letter from someone who’s not a patient, the meat is that the medium has changed, but the process hasn’t, and that’s, that’s what, that’s what we spend a lot of time. Reassuring practices is you’ve got this, you know, you know what you’re doing, you know how to deliver care. The fact that the medium’s changed, you know, a video consultation is nothing more than a phone call with pitchers. So don’t consider it to be something different. Start from a phone call, escalate to a video call, but, you know, have the reassurance that actually this is, this is channel shift. This isn’t a change in what you’re doing or how you work in and not, should it be, and where suppliers present that, then it chest, cat’s a burden. And that’s where we think the NHS deserves better. the fact is, is that those organizations are doing really, really important work and I’m so passionate about primary care. We could do the staff stuff. So if we do in lots of other industries, but we don’t, and that’s because I think primary care is a place where actually the more work we put in to help primary care, you know, that’s dividends for me in the future, that’s dividends for my family in the future. and that’s what we mean by the NHS deserves better. Do I think that there’s other suppliers that could, could do better? Absolutely. but I think the NHS is savvy enough to, to know what the one I know the need and, and vote and vote with the feet.
So my practice, during COVID they turned off III consultations. I’m not a phone person. I hate picking up the phone. I hate waiting on hold. I want access online. And I want to be able to fill out a form and get whatever I need from a doctor. and they haven’t turned it back on. And it’s really frustrating for me because I’m like, I don’t want to sit on hold for an hour in the morning to wait to be told there’s no appointments. And I, you know, I fully understand that there’s so much pressure on them, but what about when practices don’t want to put things online and they feel like they’re maybe too busy? What should our response to that?
It’s because practices are, are too busy. There’s less GPS than there had been forever before throughout Kirby, there was a, there was a big media narrative that GPS weren’t there that the front doors were closed. Believe me, the GPS were working, the working remotely, they were working in the surgery. The doors were closed because that’s what the NHS told practices to do. Practices and GP partners are working longer hours for less money. They’re not on the golf cart. They don’t have the time to do this. you know, there’s not a week where we don’t have a practice manager or a GP who’s really upset. And it, you know, he’s often on tears with us this weekend, there was four GPS on Twitter who posted pictures of bridges saying that they were going to commit suicide. It is really, really, really tough for practices, but it’s really tough for patients as well. So, you know, so, so there’s that balance there. So that’s what we do a lot around country. We call it control and managed in that. So yes, if you feel like you’re struggling, turning the consult off, turn your eConsult offer off the website completely often feels like a solution because that demand disappears, but it doesn’t disappear. It’s displaced. So we often talk to practices about, well, turn it off out of hours could be something that helps you not come into a delusion the morning, but actually that’s hidden demand that you’re doing elsewhere. Exactly. So if demands 150% and your eConsult tool is capturing 120% of it. And even if it’s reducing some of that demand, there’s still more demand than you can manage. And this is the same in any other sector. So, you know, in it support traditional kind of transactional customer service, the traditional mantra is we’ll get the demand, understand it so you can manage it and pattern it. So we do lots of work with practices to say, well, actually we can turn off. We can help them turn off certain bits of eConsult. So while an ACU on the day and need, isn’t gonna be appropriate out of hours because there’s more appropriate services, a request for a sick farm or a med review is always going to end up at the practice. So allow that to be served 24 hours. We do a lot to help practices understand that the demand isn’t coming from those tools as well. So they will see demand that they didn’t see before. And the presumption is sometimes that the tools causing the demand, that’s often not the care. So we use analytics and the website to kind of go, well, look, if you had 2000 people visit it, 25% went to a patient facing service, an appointment, booking, a prescription booking app, something like that. So many went on to use NHS choices. Aren’t, it’s just 1, 1, 1, and actually only these ones came onto usury console. So if you’ve been getting a thousand eConsults through in a day, but actually you can see that there was 3000 potential people that can help a little bit, but you know, it’s, it’s hard because practices are run by partners and practice management staff. And the partners are the ones who provide the bulk of care in surgeries because locums aren’t available other than a really high rare, which is why practice is a change in the skills mix. so it’s, you know, it’s often, it’s often really hard. You know, I’ve had conversations with my mom where she’s struggled to access primary care because she didn’t understand the right route. She couldn’t find the right button to click in the right place to get what she needed. And the presumption is that, you know, the don’t want to give you the appointments cause the don’t, you know, and that’s, that’s definitely not the care it’s the working so hard, you know, we’ve less apart than they’ve had before. Certainly less apart than the pad before from the government. The hair day of primary care funding is gone. You know, they’re asking me do more with less, you know, and this isn’t a backdrop of delivering the biggest ever vaccination program that the UK has ever seen. You know, something primary care is very good at is vaccination programs. So they’ve delivered that at scale. you know, we had 11, 11.2 million bookings for vaccinations, not through the national vaccination booking portal through our own booking polls. And that was incredibly rewarding to be able to go, well, look, you know, this is really scary. It’s a really scary time, but to go well, at least we know that we’re helping X amount of people to do that stuff. And some of what we’ve been doing around COVID is, has been really great for the team. but parties want to provide that care that they’re struggling and they need help. And you know, what can patients do to help? Well, it’s not about saying don’t visit your GP because that’s pollute. You need to visit the right place for you. but it’s important to remember what you need versus what you want, you know, so what is willing, you’re willing to work for and sh and, you know, be welcome with your practice. It’s fine to say to them, look, I’ve got this neglect concern, but I’m not asking for a response through where are actually angry to be proactive about my own med review, but don’t worry. I’m not asking for it in today. I’m just submitting it now, you know, and I’m having that conversation with the practice. it is frustrating for patients, but it’s very frustrating for practices media coverage doesn’t help because the message isn’t helping people understand. there was a lot of stuff about a and E last week, with, you know, with the, and ethics where she was saying it was, and this is the situation. And, you know, one of the national, peer has put a message out saying, you know, inability to access GP causing pressure a and E there’s absolutely no data to support that. You know, people are turning to pain because they’re acutely unwell, they’re acutely unwell because they can’t get the care they need. That is because of a multitude of reasons, mainly because the staff aren’t there mainly because the funding’s not there, it’s not because anyone is sending anyone to, and as a first point of call, nobody in Amy is happy to be in India. No one is choosing to go there, you know, for, for Giardia. So, you know, it’s an interesting time for practices, but, you know, I emphasize with patients, I do, and we do lots of, you know, the AV solutions, great for increasing accessibility and making sure people can access that stuff. But, you know, we often say we’re a primary care business and the practice teams are, really who work with the most invested in getting this part of their need. Yeah. I think we only way that it’s ever going to change is like mutual support with each of their suppliers support in NHS organizations, primary care organizations, patients understanding, practices, understanding patients. And if, if we all work together, then it’s, you know, it’s more likely to, to improve my practice. having said they turned the, the online, consultations off every time I’ve rang them. And I don’t ring my doctor often, cause I don’t really like doctors. I work in the area, but I don’t know. I find him speaking to doctors as a patient. It makes me nervous. but they, every time I’ve called them, they are on it. I’ve net, they’ve never rejected an appointment. I had to go during COVID cause I have, asthma, which doesn’t come up often, but it did during COVID worst time ever. and they saw me straight away and despite obviously having a worry, it might be COVID. They saw me, they, they, they helped me and they were great and, nothing bad to say about about it. And I feel, I really feel for them Prior to this, we will absolutely make sure people get the care they need. So, you know, I’ve had a relative, in the last two years, who’s complained massively about, you know, something they wanted around, around them ads and, you know, on the face of it, not an objectionable request, but on the face of it, not, not an issue, but as far as I could see it at the same time, I’ve had relatives who about two week comes to referrals who have been seen triaged by the practice, into the practice nurse the next day, and then through the hospital in two weeks, you know, so the care that needs to happen is there, but, you know, we’ve had a fantastic primary care system in the UK for a lot of years, you know, in other countries it would be my usual to see a pharmacy first to, to, to do more self care. And, you know, we’ve come to love and respect that, that relationship that we have with our GPS. And we want that for everything. And you know, it’s great. You know, I also have my accountant to do all my bookkeeping, but actually I’m only going to go to them for the stuff that only they can do. and it’s the, you know, it’s the same with our healthcare professionals. You know, you need to understand the skill set of GPS, understand what it is that you want from them, but understand that the supported by a wonderful practice team have a right of roles, you know, and you know, I’d be happy to see whoever they’re telling me to see, because I know that ultimately they want, you know, they want me to be well they’re in the business of making me well. Yeah. I don’t think any GP, you know, where the market has been at any point has been doing their trend and, and decided to do GP because they thought it was going to be any easier than any other specialism. It’s not, you know, and it’s not that they’re a Jack of all trades, they’re a specialist generalist, you know, and that is a skillset in its own. Right. Does GPS did that knowing the, what the we’re walking into it in primary care and knowing that that was where they were going to make an impact. And you know, I’ve got, I mean, I’ve got so much respect for, for, for, for primary care and you know, that kind of area in the market now that I don’t love taking care of hospitals are brilliant. but primary care, you know, for me that, you know, that’s what it’s all about. Yeah. You don’t go into and jump in a job like that if you don’t want to help people do so. Thanks again for joining last week, Tom, we’ll be continuing this conversation next week. So I’m looking forward to speak to you again and don’t forget to rate and subscribe wherever you get your podcasts. And if you’ve got any questions for us or our guests, please email what the hell [email protected]